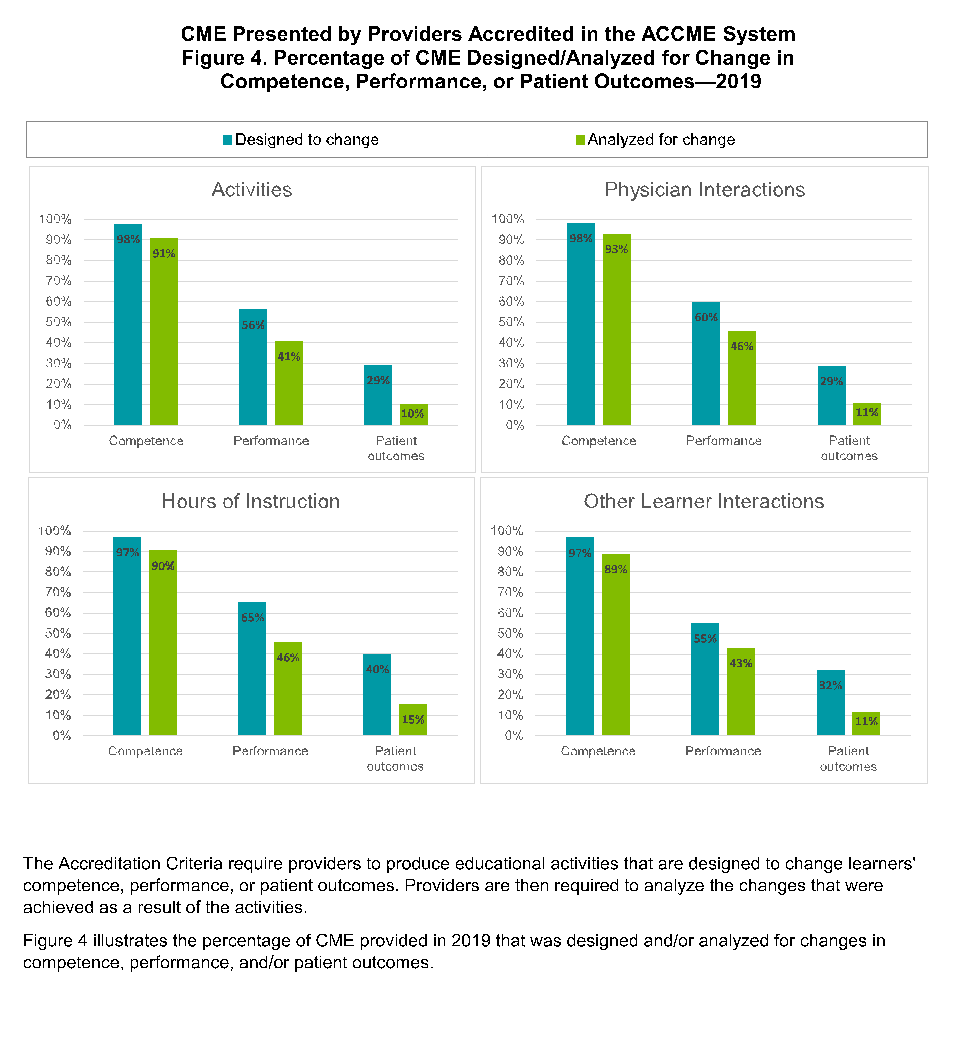
The continuing medical education (CME) market has grown significantly since I finished training. In 2010, there was $2.4B in revenue on approximately 950K offered CME activities. In 2019, 1.3M activities (27% increase) generated $3.1B in revenue (23% increase) (ACCME). Yet despite this growth, increasing regulation regarding “maintenance of certification” has become a flash point for many physicians feeling it threatens their ability to continue practice and doesn’t improve patient care. This feeling shouldn’t come as a surprise. The industry currently promotes provider competence in most of its activities. CME is not well designed to improve provider performance or drive patient outcomes despite these becoming the key performance indicators for most healthcare institutions4. (see chart)
CME is not well designed to improve provider performance or drive patient outcomes despite these becoming the key performance indicators for most healthcare institutions.
One would think this area is ripe for disruption and innovation given the large market size, the focus on outdated metrics, and the forced consumption that has been codified. However, today I complete many of the same types of courses and activities I did ten years ago. Adam Grant describes this as the “overconfidence cycle” in his new book Think Again. The pride of what we know leads to conviction and confirmation bias that ultimately validate our existing “knowledge.” His argument is that we don’t know what we don’t know, because we are not using the right tools or mindset that expand our ability to discover new knowledge2.
CME cannot be effective in its current state when the current model has no way to help healthcare providers identify these blind spots.
Our patients expect us to engage in continuous discovery. They would be surprised at the lack of innovation in CME given the advances in medical care. In my eleven years of practice, I have completed over 300 hours of continuing medical education, but I am not confident this education has been the most relevant to my practice or has improved my performance as a surgeon. At times, I was checking a box, or attending courses that confirmed what I already knew. It is also unclear that the CME I have completed has improved my patients’ outcomes. Eighty percent of medical education focuses on biology of disease, yet 60% of premature death is due to non-biologic causes, such as psycho-social determinants1. The education I have completed mirrors this, mostly focusing on treatments and techniques.
Additionally, the volume of what needs to be known is growing at a pace where it is difficult to keep up.
While it took 3.5 years for all that is known in medicine to double when I started practice in 2010, today it takes less than 2.5 months1. It is a huge challenge to face a tidal wave of information when my primary tool offers an inefficient system.
The quality of the content is also difficult to determine in a growing market of offerings. I often find courses that have experts sharing their experience. However, these courses have little opportunity for meaningful interaction that drives practice changes.
Healthcare providers search for content depending on their practice setting; CME offerings at the academic institutions are often not relevant for the community practices, forcing them to seek out quality CME at huge expense.
Large associations and specialty academies continue to dominate the CME content available, but their concept of an innovative activity is a webinar. Furthermore, the best content for me is not the same for one of my colleagues. We are all at different stages, with different practice needs. The American Academy of Orthopaedic Surgeons sends me weekly emails about their next shoulder arthroscopy course or total knee arthroplasty publication despite my practice having been 99% spine surgery for 10 years. Content that is actually curated for me and my practice would be a good start at innovating.
For CME to have a lasting impact on our patients, both now and in the future, content must also include multiple mediums and interactive techniques3. Our current infrastructure for CME is not set up to meet us where we practice. I may intend to sit down at 8pm for the 1 hour webinar, but then dinner runs late, or I forgot I was picking up my kids from swim practice that night. It continues to get pushed off. This results in a lost opportunity to improve our care. CME as a product does not fit the market; it is not fitting into our practice.
To be continued in Part B...
References:
- Densen, Peter. “Challenges and Opportunities facing medical education.” Transactions of the clinical and climatological association. 2011; 122: 48-58
- Grant A, Think Again 2021
- Marinopoulos , SS. “Effectiveness of Continuing Medical Education” February 2007 Evidence Report/technology Assessment 149(149):1-69 Johns Hopkins University
- ACCME Data report 2010 & 2019
Dr. Ian Madom, an Orthopedic Spine Surgeon and the Co-Founder of Mocingbird.
Created by Healthcare Professionals. For Healthcare Professionals.
Don’t have a Mocingbird account yet? Sign up for your free trial today at mocingbird.com!